Adolescence is defined by the World Health Organization (WHO) as the age range between 10 and 19 years. Some doctors define this phase as an intermediate period between childhood and adulthood, but the truth is that adolescence is a period of many changes in the individual’s body and mind. It is a new time, and new things always bring fears and insecurities, and give rise to doubts, desires, rebellion and anxieties. There is great concern about the social inclusion of these young people and the possibility of STDs and unplanned pregnancies.
According to a census conducted in 2002, Brazil has approximately 35 million adolescents between the ages of 10 and 19(1). The Brazilian Federation of Gynecology and Obstetrics Societies (FEBRASGO) showed that, in 1993, 22.34% of adolescents were pregnant, and this number increased to 26.96% in 1999(2). This means, indirectly, that the number of adolescents who have sex without using condoms has also increased. The fact that this group does not use condoms increases the chances of acquiring one or more STDs.
Sexually transmitted diseases are, by definition, those infectious diseases that are transmitted most commonly, or most efficiently, through sexual contact and whose transmission is of epidemiological importance(3). The WHO admits that there are more than 340 million new cases each year in the world of just four STDs (trichomoniasis, chlamydia, gonorrhea and syphilis). Complications from STDs can lead to death(4).
Currently, there has been a decrease in prejudices and repression regarding virginity, and this change has given way to encouragement, leading to greater liberation(5) and increasingly earlier sexual initiation.
Given these facts and considering that adolescence is the period in which most individuals experience their first sexual relations, it was necessary to conduct this study. Through it, we will be able to verify any changes in behavior in the profile of adolescents who were treated at the STD service at UFF, in order to always carry out preventive and educational work, and not just curative work, so that there is a reduction in the risk of contracting STDs by adolescents.
LITERATURE REVIEW
WORLDWIDE AND BRAZILIAN DATA
There are currently over one billion people in the world between the ages of 10 and 19, representing almost 20% of the world population. In Brazil, there are approximately 35 million adolescents of both sexes between the ages of 10 and 19, according to 2002 data from the IBGE (Brazilian Institute of Geography and Statistics)(1). At the International Conference on Population and Development, held in Cairo in 1994, the health and reproductive rights of adolescents and young people received special attention in paragraph E of Chapter VII, which included topics such as unwanted pregnancy, abortion and STDs/AIDS. The recommendations of this conference provide for the encouragement of responsible and healthy reproductive and sexual behavior, including voluntary abstinence and the availability of appropriate services and counseling specifically designed for this age group. Countries must ensure that medical programs and attitudes do not limit adolescents’ access to the services and information they need(6). These services should guarantee adolescents’ right to privacy, confidentiality, respect and express consent, while respecting cultural values and religious beliefs, as well as the rights, duties and responsibilities of parents. Countries should protect and promote adolescents’ right to education, information and reproductive health care, and significantly reduce the number of teenage pregnancies. Governments, in collaboration with Non-Governmental Organizations (NGOs), should establish appropriate mechanisms to respond to the special needs of adolescents. Representatives from more than 175 countries around the world have signed a document endorsing these recommendations. The Brazilian government is also a signatory to the Cairo Program of Action, having committed to implementing policies aimed at adolescents’ sexual and reproductive health and rights(6).
Data from the entire Brazilian territory, presented by the STD/AIDS Coordination of the Ministry of Health, indicate an increase in cases of STD/AIDS among young women from 1999 to 2002, in the age group between 13 and 19 years old. In 2001, there were 227 cases of infection by the
human immunodeficiency virus.(HIV) in girls versus 134 in boys. In 2002, despite the significant drop, the number of cases continued to be higher in girls, and the main route of transmission in both sexes was sexual(7, 8). Surprisingly, the greatest fear of adolescents is not AIDS, but pregnancy. Condoms have been used mainly to prevent pregnancy, and their use as a means of preventing STDs has been met with resistance by many people, who claim there is no need to use them(27), which makes them much more vulnerable to contamination by an STD or AIDS. From 2002 to 2003, the Superintendence of Public Health, of the Municipal Health Department of Rio de Janeiro, recorded an increase in the number of cases of condyloma acuminatum in the age group of 15 to 19 years(9).
Approximately 16.18% of the population of the city of Rio de Janeiro is made up of adolescents aged 10 to 19, corresponding to approximately one million inhabitants (data from 2002 – SMS/RJ)(9). This fact makes this study extremely relevant, since these young people begin their sexual life early, use condoms irregularly and have little knowledge about the reproductive cycle, as described in a study on the level of knowledge about reproduction and safe sex carried out with adolescents from a high school and elementary school in Fortaleza, Ceará(10).
In another study, it was observed that needy young people or those who lived in low-income communities were more frequently subject to behaviors suggested as risky, which had an impact on their health(27). Within this framework that makes up the behavior described above, greater sexual activity, a greater number of sexual partners and less frequent use of condoms are also included(11).
Thus, one of the main ways to contain the spread of AIDS and other STDs is to raise awareness among the population. In particular, within this specific group, providing knowledge about the methods of transmission of STDs, so that adherence to the information occurs, modifying the behavior pattern of these individuals(10,11).
The main prevention strategies carried out by health promotion programs are the provision and motivation of condom use, emphasis on the use of disposable needles and syringes, control of blood and derivatives, in addition to the adoption of care in occupational exposure to biological material, as well as in the adequate management of STDs(10).
Thus, as stated by the WHO, “Promoting the health of adolescents is one of the most important long-term investments that a society can make”(6).
ADOLESCENCE
With the growth of scientific research in the areas of human and biological sciences, there has been greater emphasis in recent decades on the study of adolescence, since it is a period in which individuals’ reproductive capacity and cognitive and social skills are acquired(12).
The term adolescent means, in its etymology,
ad (forward) and
dolescere (to grow with pain), which characterizes a period of mutation, crises, a stage of maturation, reflecting changes and a phase of transformations and reaching the social, physical and intellectual levels(12).
Its definition regarding the chronological period finds contradictions in the current literature(13).
Other concepts define this period as a phase of adaptation to secondary sexual characteristics, search for autonomy as an independent individual and, also, opening up the capacity to establish one’s own code of ethics or scale of values(13).
The need to experiment with behaviors due to biopsychosocial changes leads these individuals to be vulnerable to contracting damages and risks to their health in several dimensions(12).
Some factors, such as lack of knowledge about one’s own sexuality, curiosity about drugs, teenage pregnancy, non-adherence to contraceptive methods and the need for group affirmation, function as a means of accessing the risks of acquiring some STD(10,12,13).
Another striking characteristic of this phase is the formation of groups, which have been defined as the natural habitat of these individuals, who bring with them their own communication, formed by verbal and body language, ranging from the contesting nature to a distinct identity. The group, then, becomes a bridge between the family and society, a place of transition, a center of training for the concretization of attitudes, expression of ideas and feelings created, not welcomed or little accepted in other social spaces(12).
The word
group has other synonyms, such as
classes (representing the transition from adolescence) and
gangs (intense and permanent movement)(13).
In the search for a new identity, these individuals present a search for idols, composed of a mixture of image or beauty, or prestige or wealth or contesting ideas. Their groups present
a certain stability , as they offer delimited values, reducing the pressure of criticism, feelings of fear, inferiority, shame and guilt, emphasizing, in their components, the idea that unity is strength through the cult of self-esteem, which occurs through positive reinforcement(12,13).
In this same space, adolescents are recognized and have the chance to strengthen their sexual identity. In addition, they may display identification vehicles that make them common, such as clothing, external signs, uniforms, badges, among others. On the other hand, it is extremely important to pay attention to this group when they present antisocial tendencies, with deviant behavior, acting through excesses in transgressing the laws that organize society(12,13).
This period that oscillates between situations of calculated risk, resulting from deliberate action, and those of senseless risk, which can compromise life irreversibly, constitutes behaviors of increasing risk for STDs, including HIV infection(11).
The greatest vulnerability of these young people comes from failures or inconsistencies in the use of condoms concomitantly with high rates of sexual activity with different partners(14).
As for STDs and AIDS, this group becomes an increasing target of health education programs, where the preventive focus must be incisive and broad. Within this context, this work should propose an awareness-raising and reflective approach, carried out by a multidisciplinary team, seeking health promotion strategies with these individuals(14).
Some educational programs specifically for this group carry out recreational activities, bodywork, workshops and stage performance as teaching instruments, motivating and influencing them to express their personal experiences(10).
OBJECTIVES
GENERAL OBJECTIVE
To compare the sexual profile of adolescents treated in the STD sector/UFF in the years 1995 and 2003.
SPECIFIC OBJECTIVES
- To describe the frequency of genital infections diagnosed in this population in the years 1995 and 2003.
- To describe the behavior of adolescents treated at the STD/UFF sector in 1995 and 2003.
METHODOLOGY
A retrospective, descriptive and comparative study was conducted through the analysis of medical records of patients treated at the STD/UFF sector, from January to December in 1995 and 2003, totaling 201 and 137 adolescent patients treated, respectively, in 1995 and 2003. Data were collected regarding sex, age, age at onset of sexual intercourse, marital status, fidelity to partner, use of condoms and diagnosed pathology. A database was then created using Excel 5.0. The results were summarized in tables and graphs and compared and confronted with those of national and international literature. The data were statistically treated using Epiinfo 3.2.
INCLUSION CRITERIA
Patients aged 11 to 19 years were included in this study. Only duly completed medical records were considered for analysis, excluding those with three or more missing relevant data.
EXCLUSION CRITERIA
Patients under 11 and over 19 years of age were excluded from the study.
RESULTS AND DISCUSSION
In 1995, of the total of 1,187 patients treated at the STD/UFF sector, 201 were adolescents, which represented 16.9% of the total number of patients treated. In 2003, of the total of 530 patients treated, 136 were adolescents, which represented 25.6% of the total number of patients treated. This data shows that adolescents sought care more in 2003 than in 1995.
We observed that in 1995, there was a greater demand for care by female patients than by male patients, respectively, 72% and 28% of the treatments performed for adolescents. In 2003, we observed a change in this data, with a greater demand for male patients than in the previous year, representing a share of 54% of adolescent care, while the demand in 2003 for female patients fell from 72% to 46% of the total number of adolescents treated (Figure 1).
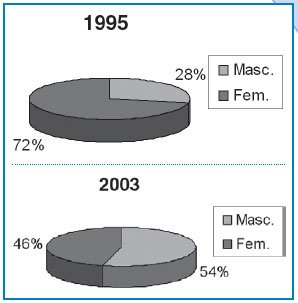
Figure 1 – Distribution of adolescents treated in the STD/UFF sector in 1995 and 2003 by sex
Regarding the age range of adolescents who sought care in both years, the demand was greater the older the age range considered equally in 1995 and 2003. There was a predominance of the 17 to 19 age range in both years, with a significant proportion of men in 2003, greater than in the previous year and greater than that of women in the same year. The opposite was observed in 1995, when the largest proportion of adolescents attended in this age range were women (Figure 2).
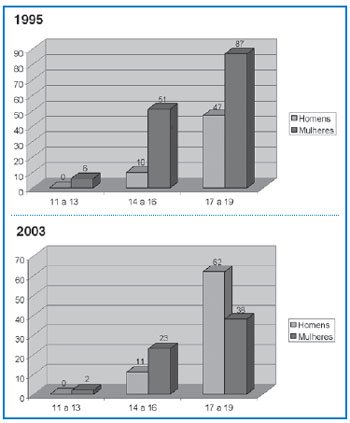
Figure 2 – Distribution of adolescents treated in the STD/UFF sector in 1995 and 2003 by age group
The age of first intercourse, reported by the adolescents attended, maintained the average age range of 14 to 16 years for both men and women in the two years observed, but we noted an increase in the year 2003 in the age range of 11 to 13 years, both for male and female adolescents, compared to the distribution in this same age range in the year 1995 (Figure 3).
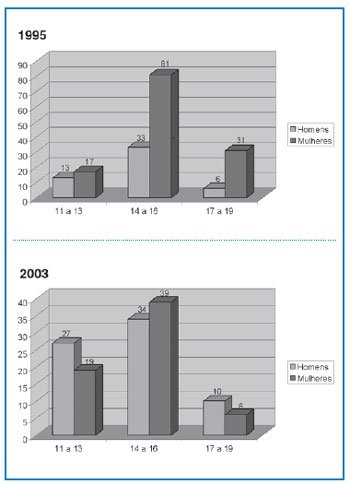
Figure 3 – Distribution of adolescents treated in the STD/UFF sector in 1995 and 2003 by age at first sexual intercourse
The marital status of adolescents showed an increase in married individuals seeking the service in general, with an increase in the percentage from 2% in 1995 to 7% in 2003 (Figure 4). This increase occurred at the expense of female patients (Figure 5). Regarding single adolescents, in 1995 we observed a predominance of females, which was the opposite in 2003, with a predominance of single male adolescents.
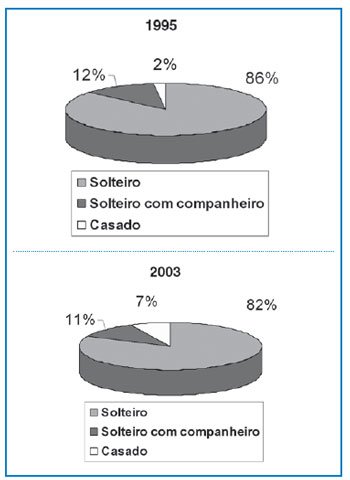
Figure 4 – Distribution of adolescents attended in the DST/UFF sector in 1995 and 2003 by marital status Figure 5 – Distribution of adolescents attended in the DST/UFF sector in 1995 and 2003 by marital status – men and women

Fidelity among adolescent patients showed an increase in exclusive steady partners, rising from 45% in 1995 to 55% in 2003, still mainly among women, but with a significant increase in men with exclusive steady partners compared to 1995 and 2003. The number of adolescents treated regarding multiple partners (three or more partners) fell from 25% in 1995 to 19% in 2003, but remained higher among men in both years observed. The number of steady but non-exclusive partners fell from 18% in 1995 to 11% in 2003, with a higher number of men reporting (Figures 6 and 7).

Figure 6 – Distribution of adolescents attended in the STD/UFF sector in 1995 and 2003 by partner fidelity
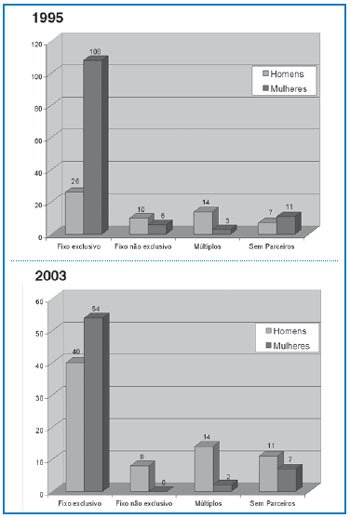
Figure 7 – Distribution of adolescents attended in the STD/UFF sector in 1995 and 2003 by partner fidelity – men and women
There was practically no change in behavior among the adolescents served in the sector regarding condom use. Most adolescents do not use them, as we can see in both 1995 and 2003 (Figures 8 and 9).
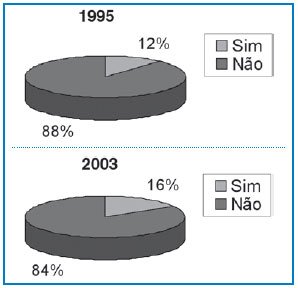
Figure 8 – Distribution of adolescents attended in the STD/UFF sector in 1995 and 2003 by condom use
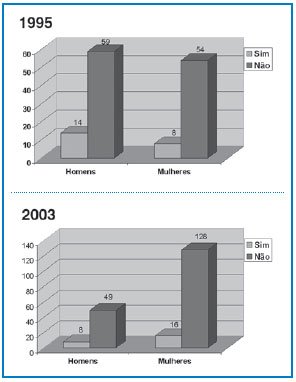
Figure 9 – Distribution of adolescents attended in the STD/UFF sector in 1995 and 2003 by condom use – men and women
Regarding diagnosis, in 1995, we observed a predominance of HPV, followed by diagnosed gonorrhea and syphilis. In 2003, we observed the same distribution of pathologies, with an increase compared to 1995 of HPV, both in men and women (Figure 10).
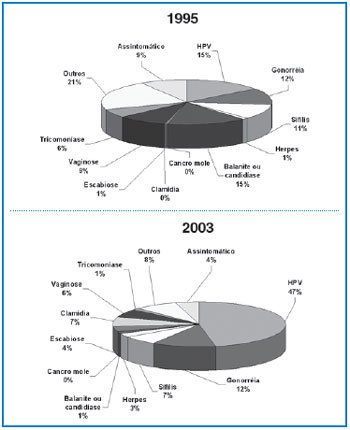
Figure 10 – Distribution of adolescents treated in the STD/UFF sector in 1995 and 2003 by diagnosis
We can conclude that, regarding the profile of this population, certain changes occurred and some trends remained.
First, the distribution of male patients seeking care increased, but the age group maintained a greater demand the older the age group considered.
The age of first sexual intercourse reported by adolescents shows us that first sexual intercourse was earlier for both men and women.
There was an increase in the frequency of married adolescents seeking care, but the single population of both men and women maintained a high demand.
Fidelity to partners reported by adolescents showed an increase in exclusive steady partners, maintaining a high distribution of this category. There was also a reduction in the report of multiple partners.
There was practically no behavioral change regarding the use of condoms. Most adolescents continue not to use condoms, a fact that should be reviewed with a view to preventing STDs.
HPV was the most frequently diagnosed pathology in 2003, both in men and women, showing a significant increase in distribution compared to 1995. Gonorrhea continues to be a pathology most frequently diagnosed in men and syphilis maintained an equivalent distribution between men and women in the two years considered.
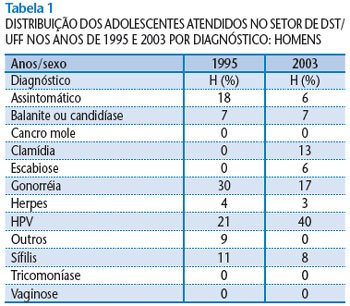
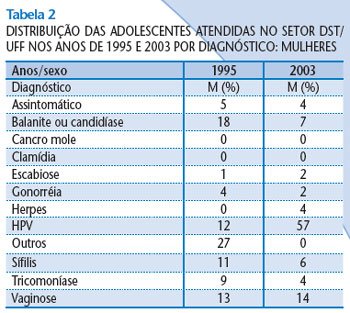


 Figure 6 – Distribution of adolescents attended in the STD/UFF sector in 1995 and 2003 by partner fidelity
Figure 6 – Distribution of adolescents attended in the STD/UFF sector in 1995 and 2003 by partner fidelity