INTRODUCTION
It is estimated that in industrialized countries, 10% to 20% of all children and adolescents have some chronic disease(1). This implies the need to adapt to the new reality of life, with restrictions such as the use of medications that sometimes cause adverse effects capable of even altering the physical appearance of these young people, causing progressive dependence on family members or making them consider themselves a burden to the family. In addition to adherence to treatment, which should always be reinforced by the professional.
Working at the Secondary Care Outpatient Clinic of the Center for Studies on Adolescent Health at the Pedro Ernesto University Hospital of the State University of Rio de Janeiro (NESA/HUPE/UERJ), the authors, as nursing residents and preceptors, observed a large number of adolescents, aged between 12 and 20 years, treated in various specialties, who presented chronic pathologies such as systemic arterial hypertension (SAH), systemic lupus erythematosus (SLE), juvenile rheumatoid arthritis (JRA), kidney disease and heart disease.
Adolescence is the stage of life in which intense biopsychosocial changes occur, when the adolescent moves towards adulthood constantly questioning the reality around him/her, as well as the phase in which the discovery of sexuality occurs. Thus, when a person discovers that he or she has a chronic disease, it has a very limiting impact on the course of his or her life, especially due to the need for successive hospitalizations – sometimes prolonged – and the absence from school.
At the residence, our greatest contact was with adolescents with rheumatic diseases who were seen on Mondays and Fridays at the NESA outpatient clinic. Based on this fact, the objective of this study was to outline the profile of adolescents with rheumatic diseases who were seen at the aforementioned outpatient clinic from January 2005 to December 2006.
This work provides a different perspective on adolescents, with special relevance for training schools, since it is believed that this work can be discussed during the undergraduate course, allowing for the training of more qualified professionals with regard to adolescents and their specificities, as well as pathological adolescence.
Furthermore, it can serve as an instrument for evaluating the care provided to adolescents, which will allow for practical reorientations as the results are forwarded to NESA.
METHODS
The nature of this study is quantitative, therefore, for its implementation, authorization was requested from the Research Ethics Committee of the Pedro Ernesto University Hospital (CEP/HUPE) through the National Information System on Ethics in Research involving Human Beings of the Ministry of Health (SISNEP/MS)(2).
The chosen setting was the Floriano Stoffel Pavilion (PFS), a building attached to HUPE, where the NESA Secondary Care Outpatient Clinic operates, located at Avenida 28 de Setembro, 109 (back), in Vila Isabel, Rio de Janeiro.
The study sample consisted of 108 adolescents, aged between 12 and 22 years, who were followed at the NESA outpatient clinic from January 2005 to December 2006.
To meet our objectives, data collection was performed manually in December 2006, January and February 2007, by consulting medical records (secondary data), using a previously prepared instrument (form) with seven questions about sex, age, education, origin, medical diagnosis, drug treatment and need for hospitalization due to rheumatic disease.
Figures and tables were used to sample the data and, to understand the data obtained, descriptive analysis was adopted, which consists of observing, describing and classifying, seeking the predominance and characteristics of the phenomenon(3).
RESULTS AND DISCUSSION
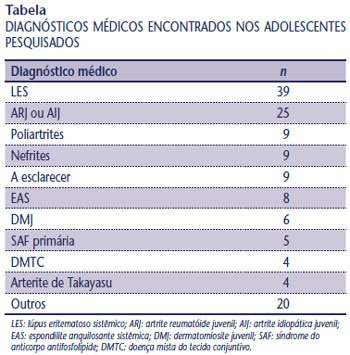
Of a total of 108 adolescents investigated, it was found that 71% were female (77) and 29% were male, which in absolute numbers represents 31 boys (
Figure 1 ).
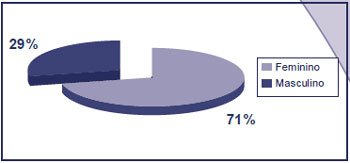
Figure 1 – Distribution of adolescents surveyed by sex
Moreira and Carvalho(4) state that most autoimmune rheumatic diseases are more prevalent in females, with this predominance being more notable in age groups compatible with sexual fertility, that is, when there is abundant estrogen secretion(4).
We recognize that the consequences for adolescents regarding body image greatly affect social relationships and sexuality, since some treatments cause changes in the menstrual cycle and facial contours (cushingoid face), alopecia, swelling, and restrictions on sun exposure. These factors go against the appeals of modernity: tanned bodies, long, silky hair, praise for a defined body, among others.
Figure
2 shows that in relation to age: 46% were between 15 and 17 years old; 37%, between 18 and 20 years old; 14%, between 12 and 14 years old and 3%, over 21 years old.
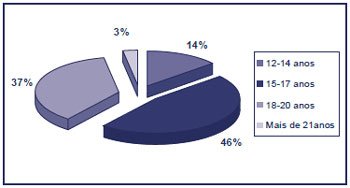
Figure 2 – Distribution of adolescents surveyed by age group
At NESA, adolescents are treated until they are 20 years old and then referred to the adult rheumatology clinic at HUPE itself. In most cases, this does not always happen immediately, due to the close relationship that adolescents establish with professionals in establishing the bond of trust between professional/user/family.
According to
Figure 3 , 38% have incomplete elementary education. Elementary education is understood as education from first to eighth grade, according to the 1996 Law of Guidelines and Bases that regulates education in Brazil. During data collection, we identified that all of them are either in the fifth grade or more advanced in this stage, which comprises eight years of education. The remaining 37% are attending high school, which in total comprises three years.
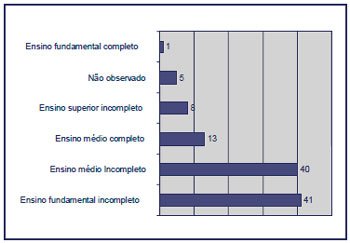
Figure 3 – Distribution of adolescents surveyed by level of education
The sample shows that the adolescents have a regular and continuous level of education, even though they are still in the formative phase. We believe that this contributes to a better understanding of their own illness, leading them to understand with ease and even question the condition they present, improving adherence to the proposed treatment.
The role of health professionals in encouraging study is also important, understanding the need for school space for social interaction.
Figure
4 shows the origin of the adolescents in relation to the distance between the municipality where they live and the care unit.
Figure 4 – Distribution of adolescents surveyed by origin
It is known that among the principles of the Unified Health System (SUS) are the regionalization and hierarchization of services, which must be organized in levels of increasing technological complexity, as well as arranged in a delimited geographic area and with the definition of the population to be served. This implies the capacity of the services to offer a given population all types of assistance, in addition to access to all types of available technology, enabling an excellent degree of resolution(2).
The adolescents in the study are distributed as follows, according to their residence: 57 (the majority) live in the city of Rio de Janeiro; 12, in Duque de Caxias, a city in Baixada Fluminense close to the capital with easy transportation – an intercity bus line that provides direct access to HUPE; six in Nova Iguaçu; five in São Gonçalo; two in São João de Meriti; and two in São Pedro da Aldeia – the city furthest from our service.
The long distance between the home and the clinic is possibly a factor that limits treatment, since most adolescents come accompanied by at least one of their family members, which implies greater financial costs with transportation.
The
Table lists the main rheumatological pathologies found in the sample of this study. The cases of SLE and JRA (39 and 25, respectively) stand out, as they prevail in greater numbers compared to the other pathologies. It is known that, even though their etiology is unknown, they act chronically and encompass a group of diseases called autoimmune.
Although the highest incidence in our country is SLE (39 cases), the Brazilian Society of Rheumatology (SBR)(6) considers it the third most frequent disease in our pediatric rheumatology clinics, followed by rheumatic fever and juvenile idiopathic arthritis (JIA). The real incidence of SLE is unknown in our country. Data from countries in North America, Europe and Japan indicate that approximately 0.3 to 7 in every 100 thousand children and adolescents have this disease.
According to Moreira and Carvalho(4), in Brazil it seems that JIA is not a rare disease, representing the second most frequent rheumatic disease in childhood.
Regarding treatment (
Figure 5 ), oral drug therapy is the most used, with 49% showing a good response to the symptoms manifested; then, we found the association of oral and intravenous medications for treatment (27%), with pulse therapy (use of methylprednisolone) and infliximab (medication that reduces inflammatory activity).
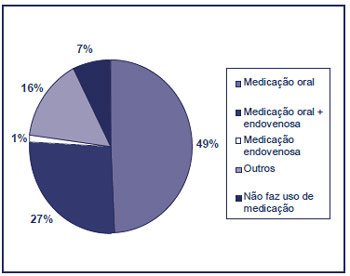
Figure 5 – Distribution of adolescents surveyed in relation to the medication used
Other types of medication administration, such as subcutaneous, topical, intramuscular, isolated or combined with oral and/or intravenous, to improve the existing symptoms, account for 16% of the sample.
Of the 108 adolescents surveyed, only eight (7%) do not use any type of medication. This leads us to consider that they may be in remission of the disease activity, clinically and laboratory stable; that the diagnosis has not yet been established, remaining without medication; or that they are adopting other types of treatment, such as thermotherapy or cryotherapy, physiotherapy, acupuncture, etc.
We can also make a pertinent analysis of the impact that the use of medications represents in the life of the adolescent and his/her family. These impacts may be financial, when it is not possible to obtain the medications entirely through the SUS; physical: organic changes (mentioned several times in this study); educational: impairment of school attendance; and cultural: need to adapt specific schedules for taking the medication.
Regarding the need for hospitalization, 54% of adolescents were hospitalized at least once during treatment, and 46% did not require any hospitalization, which in absolute numbers means that 58 adolescents were already hospitalized, while 50 were not. These data are well balanced (
Figure 6 ).
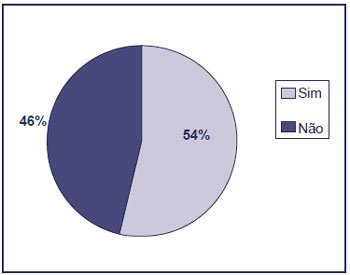
Figure 6 – Distribution of adolescents surveyed by hospital admission
When analyzing this data, we can consider that:
- some adolescents have tertiary care as their entry point into the service;
- some teenagers need to be hospitalized to undergo more complex, invasive procedures with greater safety;
- Some adolescents do not adhere to therapy effectively and present complications in various organic systems. Even with full adherence to treatment, some cases do not show good progress.
CONCLUSION
Based on the data presented, we conclude that we achieved the objective proposed in this study by identifying the profile of adolescents with rheumatic disease treated at NESA. Furthermore, we understand that outpatient care should be a time when adolescents should feel welcomed and their health demands met, which are not always the visible and palpable physical and symptomatic borderline demands. Therefore, it is necessary to understand them as unique and individualized beings.
Regarding the specificity of our care, we believe that, as an art and science, nursing has a broader view of the issues involving adolescents with any chronic disease. In this process, interdisciplinary work is essential for the care of these adolescents, with consultations, health education groups, providing a space for greater interaction between adolescents, families and service, in addition to occupational activities that can be provided.
We can consider that the search for care at NESA is due to it being a reference service for adolescents widely known in the state of Rio de Janeiro and university care, at all levels of care, with quality and responsibility.