INTRODUCTION
Adolescence is characterized by being one of the fastest phases of human development. In addition to physical and biological transformations, adolescence is also characterized by a period of physical, psychological and social vulnerability with complex changes. However, it is necessary to consider an important fact: both biological, psychological and social development will depend on the sociocultural context in which the adolescent’s family is inserted, thus outlining its possibilities and limitations
1 .
The World Health Organization (WHO) defines the chronological limits of adolescence as 10 to 19 years of age, that is, the second decade of life
2 . This criterion is adopted in Brazil by the Ministry of Health and the Brazilian Institute of Geography and Statistics (IBGE).
It is estimated that adolescents represent 18% of the world population
3 . In Brazil, adolescents represented 17.91% of the Brazilian population in 2010, a figure that corroborates the global estimate. Analyzing demographic data, it can be seen that Brazil is experiencing a decline in the number of adolescents: in the 2000 census, adolescents represented 20.78% of the Brazilian population, in the 1991 census they represented 21.82% and in the 1980 census they represented 23.38%
4 .
Several authors and official publications highlight the complexity of adolescence
5-6-7-8 , where adolescents go through a dynamic process of maturation. It is a phase of great physical transformations concomitantly with the emergence of new cognitive abilities.
Their new role in society brings with it a constant questioning of values. All these changes result in a predisposition to new experiences testing attitudes and situations that may threaten their present and future health, such as: accidents, unplanned pregnancy, sexually transmitted diseases, drug use and eating disorders
6 .
According to the WHO, mortality rates in adolescence are low compared to other age groups, and have shown a slight decline in the last decade. Globally, the leading causes of death among adolescents are traffic accidents, AIDS, suicide, lower respiratory infections and interpersonal violence
2 . A study conducted by the United Nations Children’s Fund in 2011 also points out that risks to the survival and health of adolescents have several causes, including accidents, AIDS, early pregnancy, unsafe abortions, risky behaviors, mental health problems and violence
3 .
In Brazil, the causes of adolescent mortality have been a concern that has plagued public health for some time
9-10-11. The vulnerability and risks to which this age group is exposed demonstrate that a large number of adolescents have their lives interrupted, with morbidity and mortality being the central external causes of this fact
12 . This study aims to perform a descriptive analysis of the epidemiological profile of adolescent mortality in Brazil in the five-year period from 2008 to 2012. The proposed analysis aims to give visibility to the issue so that more effective actions can be directed to public policies aimed at guaranteeing adolescents the right to life.
METHODS
This is an observational, descriptive, retrospective epidemiological study, based on secondary data obtained from DATASUS – Mortality Information System (SIM). This system is managed by the Department of Health Situation Analysis, of the Health Surveillance Secretariat of the Ministry of Health, in conjunction with the State and Municipal Health Secretariats. The Health Secretariats collect Death Certificates from the registry offices and enter the information contained therein into the SIM. One of the essential pieces of information is the underlying cause of death, which is coded based on the information declared by the attesting physician, according to rules established by the WHO.
Data on adolescent mortality in Brazil were collected. Since the WHO establishes that adolescents are included in the age range of 10 to 19 years, two age groups were selected in DATASUS: one from 10 to 14 years, and another from 15 to 19 years. The path followed in the database was DATASUS – Health Information (TabNet) – Vital Statistics – Mortality
4 . In SIM, death certificates are coded using the 10th Revision of the International Classification of Diseases – ICD-10. For this analysis, deaths by residence were considered, that is, the number of deaths counted according to the place of residence of the deceased.
The time series analyzed was from 2008 to 2012 because these were the years in which the demographic and socioeconomic data of the resident population were published in full on the DATASUS portal, thus allowing the calculation of the specific mortality coefficient by age group in the national territory and in each federative unit. For comparison purposes, demographic data of the resident population from other years were used. All data for this study were extracted from the DATASUS portal
4 .
The socioeconomic variables studied were: sex, color/race, education and marital status.
The cause of death was analyzed according to the chapters of the ICD-10. Chapter XX of ICD-10, which refers to external causes of morbidity and mortality, was detailed using the list of elements of ICD-BR-10. The data collected were tabulated using an electronic spreadsheet (Excel
®
program2010 version). This study uses descriptive statistics and calculation of the age-specific mortality coefficient for data analysis.
This research uses only secondary data from a public domain database. For this reason, it is exempt from the need for approval by a Research Ethics Committee, as recommended by Resolution No. 466/12 of the National Health Council (CNS).
RESULTS
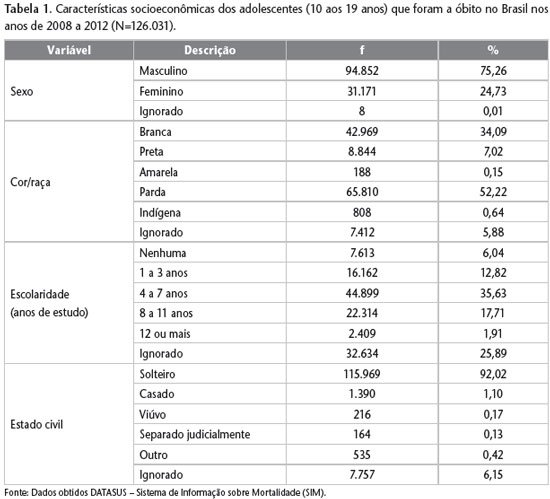
In the time series analyzed, 126,031 deaths of adolescents were recorded in Brazil. The year 2012 was the year with the highest number of deaths recorded in this population, accounting for 26,979 deaths. Based on the data analyzed, it was found that deaths of adolescents represented, on average, 2.22% of the total deaths of the Brazilian population. In previous five-year periods, from 2001 to 2005, adolescent deaths accounted for 2.56% of all deaths in Brazil, and in the five-year period from 1996 to 2000, these deaths accounted for 2.78%.
Table 1 shows the socioeconomic characteristics of adolescents who died in Brazil during the study period. It can be seen that male adolescents account for 75.26% of this population, and brown skin color was predominant in 52.22% of cases. The highest frequency of education of the population was 4 to 7 years of study, which represented 35.63%, with the second highest frequency being recorded for the ignored item (25.89%). Adolescents who died during the period were predominantly single (92.02%).
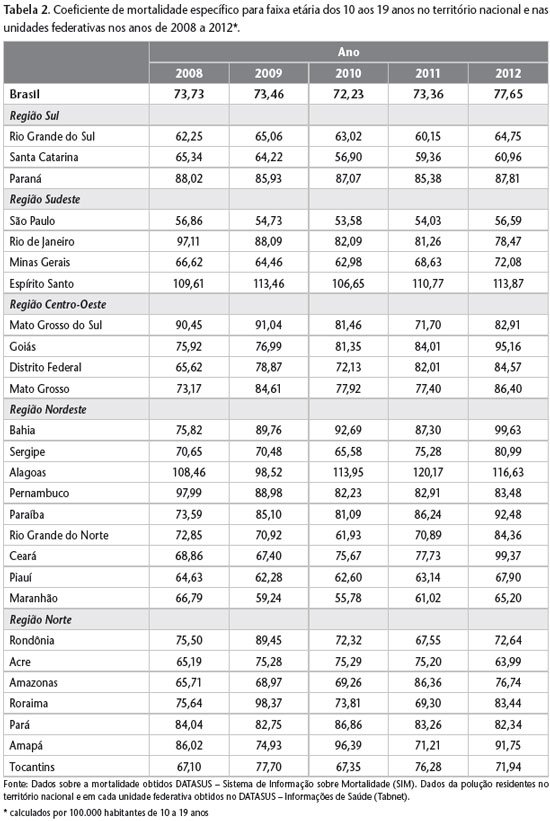
The age-specific mortality rate, calculated per 100,000 inhabitants aged 10 to 19, was higher in 2012 than in the other years of the series, with a considerable increase from 2011 to 2012, when this rate went from 73.36 to 77.65. When the age-specific mortality rate is analyzed by federative units, it was found that the state of Paraná in the southern region, Rio de Janeiro and Espírito Santo in the southeast region, Bahia, Alagoas and Pernambuco in the northeast region and the state of Pará in the north region presented a rate above the national rate in all years analyzed. The state of São Paulo presented the lowest rate in all years analyzed. In 2008 and 2009, the highest coefficient was recorded in the State of Espírito Santo, while in 2010, 2011 and 2012 the State of Alagoas recorded the highest number of adolescent deaths in relation to the population in this age group (Table 2).
Deaths from external causes of morbidity and mortality, included in chapter XX of ICD-10, are identified as the main cause of death among adolescents in Brazil. External causes accounted for 66.25% of deaths among the population aged 10 to 19 in the time series analyzed. The second most frequent cause of death among adolescents was neoplasms, chapter II of ICD-10, with 6.56%. These data are shown in Table 3.
External causes were analyzed in detail using the list of elements from ICD-BR-10. It was identified that aggression represented 51.62% of deaths due to external causes in the period analyzed, followed by traffic accidents (25.62%) (Table 4). The year 2012 was the year in the time series in which the highest frequency of deaths due to aggression occurred in the period, representing 36.45% of the total deaths of adolescents in the year.
Table 4 also shows the frequency of external causes, detailed by the list of elements of ICD-BR-10, separated by male and female genders. It can be seen that males are affected much more frequently than females in deaths from external causes. The involvement of males in deaths from external causes was 85.24%, while that of females was 14.76%.
DISCUSSION
This study found the alarming fact that 66.25% of adolescent deaths are caused by external causes, chapter XX of ICD-10. External causes are traumas, injuries or any other health problems – intentional or not – with sudden onset and as an immediate consequence of violence or another exogenous cause
13 . Assaults are included in this chapter and are the main cause of death among external causes of morbidity and mortality. In 2012, 36.45% of adolescents between the ages of 10 and 19 died as a result of assault. When we compare this percentage with that of the total population (4.8%), we see a shocking difference
12 .
Minayo
14 states in his study on violence in adolescence that the preferred victim of homicides is the young, non-white, poor, male, with an average age between 15 and 18 years old, living in the outskirts or urban slums, usually killed by a firearm projectile and referred to as criminals in police records. In this analysis, we can see the predominant involvement of males in external causes, especially in assaults, which include homicides. The other socioeconomic variables listed by Minayo were not analyzed specifically for external causes in this study.
Judging by the data found in this analysis, we can describe the profile of adolescents who die in Brazil: they are predominantly male, of mixed race, with 4 to 7 years of formal education, single and victims of external causes of morbidity and mortality. The finding that the main determinants that kill our adolescents are outside of strictly medical procedures
14 generates the feeling that this scenario can be changed. However, this phenomenon is not exclusive to Brazilian society. The great vulnerability of adolescents to death from external causes, especially male adolescents, has been described in several other studies with data from the reality of Brazil and the world
9-15-16-17-18 .
The age-specific mortality rate was calculated for the national territory and for each federative unit, enabling a general and fragmented view of the Brazilian scenario, respectively. This way, it is possible to verify the places where adolescents are most vulnerable. Identifying this reality is essential for decision-making by the management. It can be seen that São Paulo presented the lowest age-specific mortality rate in all years of the time series. When analyzing the lethal violence to which adolescents are exposed through the 2012 Adolescent Homicide Index, it was noted that São Paulo, the most populous state in the country and with a large number of large municipalities, had the greatest drop in this rate in recent years. This phenomenon was not restricted to the capital, but expanded to a group of municipalities in the state
12 .
The Unified Health System (SUS) has had adolescent health care programs for decades. The essence of the SUS is the practices of disease prevention and health promotion. However, in the age group between 10 and 19 years, there is an increase in problems that could be avoided by these measures. Given this scenario, the viable and coherent alternative is to change the emphasis of health services aimed at adolescents. Health professionals should include preventive measures as a fundamental component of their care practice, instead of strictly biological and curative care. Health promotion activities aimed at the young population are more effective when developed from a collective health perspective, as they consider the individual within their context. This approach facilitates the approach to the problems of this population, such as early sexual activity, peer pressure, drug use, accident prevention and urban violence. Internationally, health promotion is the term used to describe interventions that allow adolescents to acquire competence and confidence in self-management of their lives
6 .
The data for this analysis are secondary data obtained through the SIM, which was created in 1975 with the main objective of providing support for outlining the mortality profile in the country, and has had national coverage since 1979
16 . Data from mortality statistics are affected by several sources of error, but from an epidemiological perspective, they provide valuable information on the health status of populations. The use of data depends, among other reasons, on the adequate completion of records, on the accuracy in determining the underlying cause of death
19. The recording of deaths by SIM and the quality of death certificate completion have improved significantly throughout the country. Deaths due to external causes, in particular, are subject to mandatory referral to forensic medical institutes, where death certificates tend to be better completed
20 . The improvement in the quality of vital statistics allows information and its respective analyses to bring about positive changes in the population’s living conditions, as they have the opportunity to provide support to managers in the processes of planning actions and decision-making.
However, even though it is possible to celebrate better performances in vital statistics in Brazil, this analysis found that there are aspects of the records that need to be improved, such as the variable of education. This item was ignored in 25.89% of the records in the time series analyzed. The incomplete completion of the variable of education in vital records was also observed by Soares Filho et al.
20 , who point out that this variable offers more reliable and less fluctuating information than average monthly income to define the socioeconomic level of the population. Lack of information on education or any other variable that one might consider may lead to erroneous conclusions, hindering the monitoring of events in the population.
CONCLUSION
This descriptive analysis of the mortality profile of adolescents in Brazil shows that the lives of most Brazilian adolescents are cut short by external causes of morbidity and mortality. In order for Brazilian adolescents to have their right to life guaranteed, this issue must be prioritized on public agendas. Alerting the population and public administrators is essential so that the dimensions of the problem of lethal violence against adolescents can be changed.
The greatest success in reducing the mortality of adolescents who are victims of external causes involves a question of intersectoral coordination. From this perspective, the SUS constitutes an important space for the prevention of diseases and the promotion of health in its broadest sense.




